Here are the options available to patients
-01.png)
This surgery reduces the volume of the stomach and restricts the amount of food you can eat per meal. Since the stomach is now smaller, you feel full much faster. Surgeons use laparoscopy for this type of surgery. They use small incisions, rather than a long one, through which they introduce long-handled instruments which allow them to make the changes to the stomach. They also introduce a tiny camera through an incision to view the site intervention on a video screen. Then they cut about 70 to 80% of the stomach with an instrument that places tiny staples and severs tissue, creating the new long and narrow gastric pouch (the size of a banana) which will now limit the amount of food that you can take while having satiety-influencing metabolic effects. You will still need to take vitamin supplements and calcium for life thereafter.
With a "Sleeve",
you should lose 50-60% of your excess weight
POSSIBLE COMPLICATIONS
- - Bleeding
- - Trauma
- - Infection
- - Leak of the stapled line
- - Peritonitis (infection of the abdomen)
- - Stricture of the stomach (stenosis)
- - Stomach enlargement
- - Additional surgery
- - Complication cardio-pulmonaire ou trombe-embolique
- - Dénutrition, carences vitaminiques, protéiques ou en micro-nutriments
-01.png)
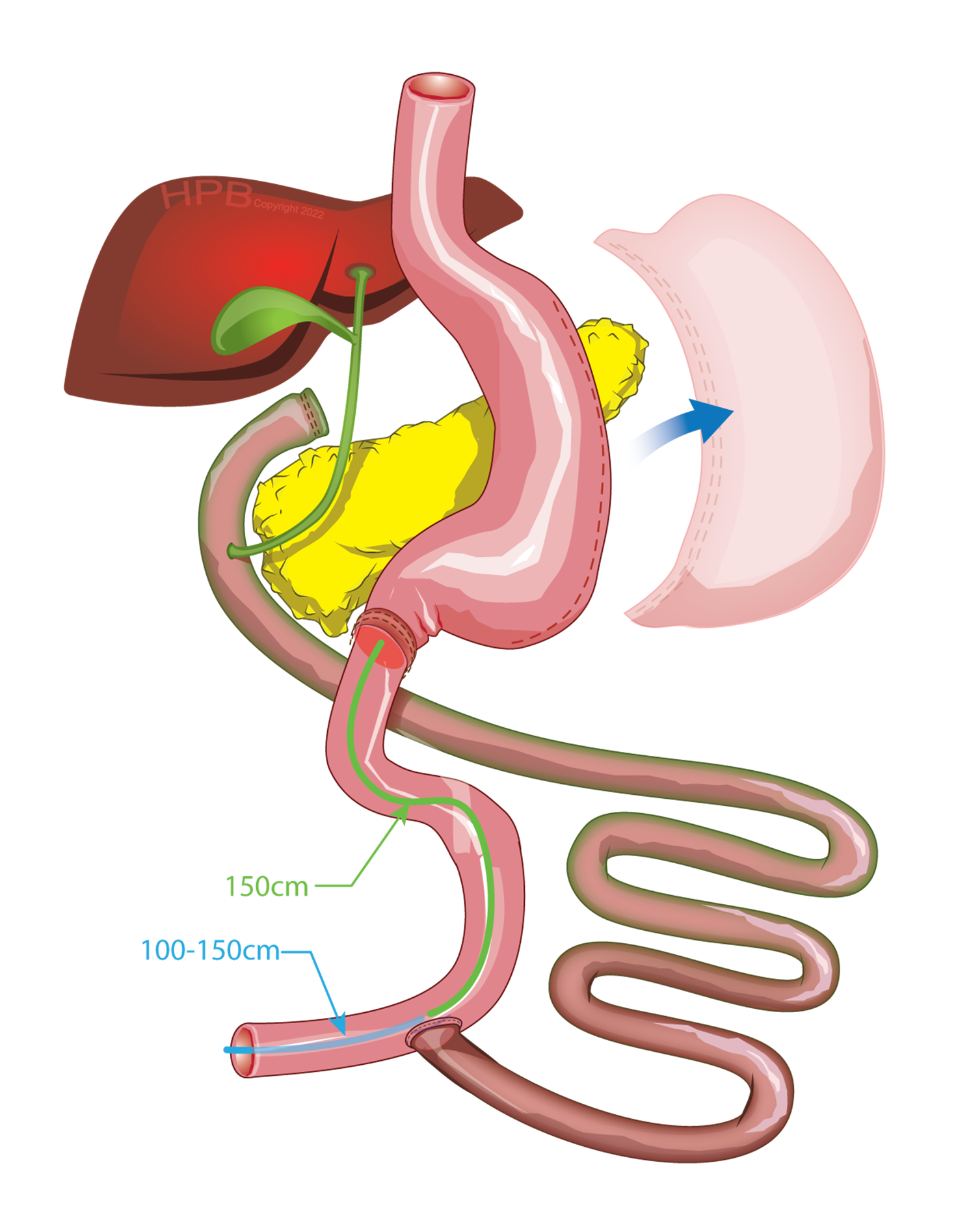
Gastric bypass reduces stomach volume and restricts the amount of food you can eat per meal.
Because your stomach is smaller, you feel full much faster. In addition, a kind of short-circuiting of the intestine is created, so food is only absorbed over only part of the length of the small intestine, which reduces absorption. The malabsorption effect is more marked on vitamins and micronutrients and this is why this procedure generally requires more sustained vitamin supplements throughout your life.
Surgeons resort to laparoscopy for this type of surgery, that is to say, they make small incisions, rather than a long one, through which they introduce long-handled instruments that allow them to make the changes to the stomach and intestine. They also insert a tiny camera through an incision to view the procedure site on a video screen. Then, they cut the stomach with an instrument that puts staples in place and cut the tissues, creating the new gastric pouch (the size of an egg) which will now limit the amount of food you can take. Once the stomach has been modified in this way, they cut the intestine about 50 to 100 cm from its beginning and connect it to the small stomach. The food then fills the tiny stomach quickly and follows a shorter route through the intestine.
With gastric bypass (Bypass), you should lose 60-70%
your excess weight
POSSIBLE COMPLICATIONS
- - Bleeding
- - Infection
- - Stapled line or anastomotic leak
- - Peritonitis (abdominal infection)
- - Stricture of the stomach (stenosis)
- - Internal hernias
- - Dumping syndrome
- - Cardiopulmonary complication or trombembolic
- - Malnutrition, vitamin, protein or micronutrient deficiencies
- - Stool changes like diarrhea and constipation
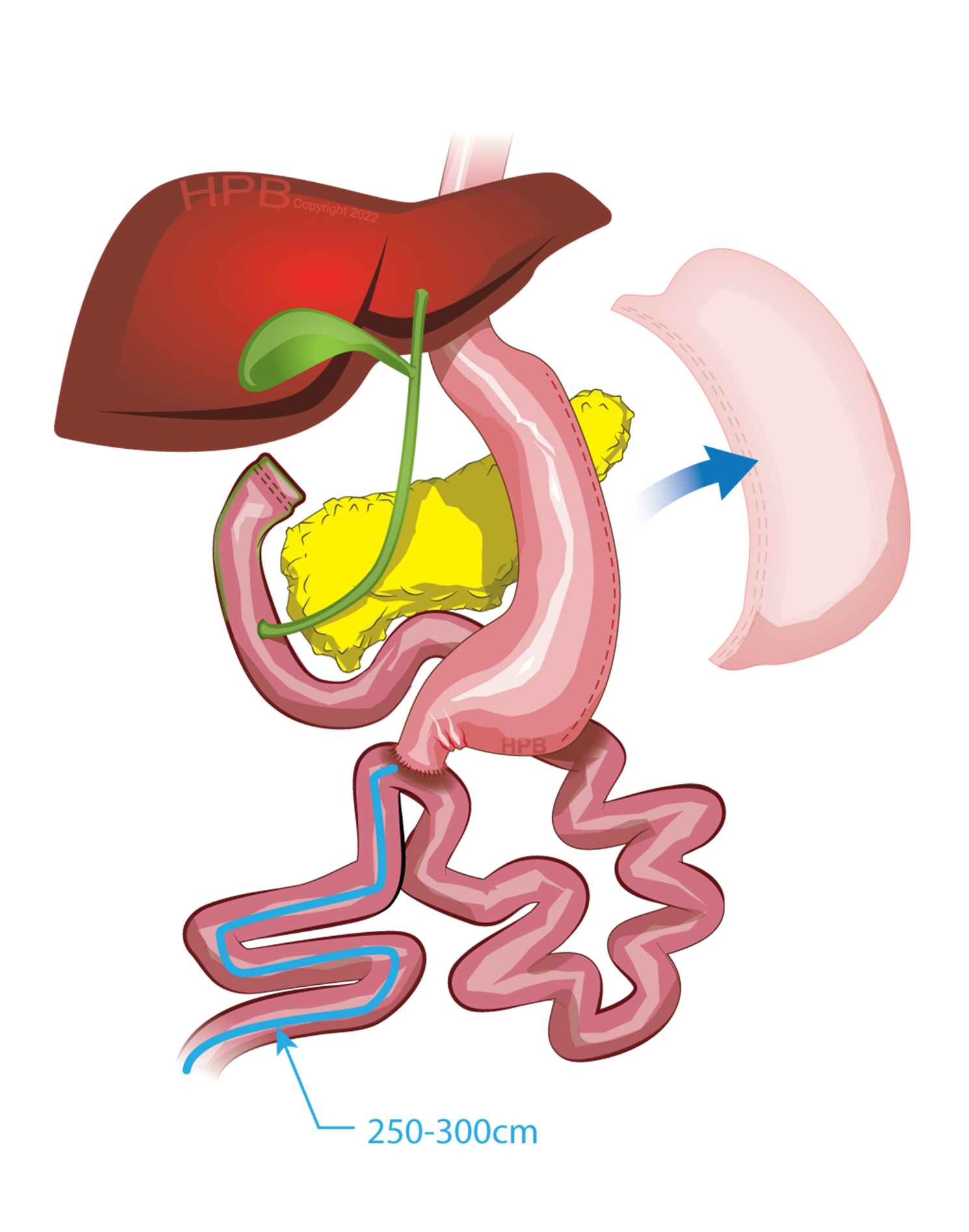
Biliopancreatic diversion is a more aggressive metabolic surgery. It combines vertical gastrectomy (the sleeve gastrectomy) with a post-pyloric intestinal “bypass”. The intestinal assembly can be of classic form with 2 anastomoses: BPD-DS - Duodenal switch. We favor the slightly less aggressive single anastomosis assembly of the SADI-S type. The ability to eat is reduced and controlled malabsorption is induced because much of the small intestine is short-circuited. A large portion of the intestine carries biliopancreatic secretions (secretions from the liver and pancreas to digest) alone without food. The final portion of your small intestine will absorb essential nutrients for your proper functioning, but this surgery is not offered to all patients. It is usually done in 2 steps. Malabsorption is significant and can lead to increased stool frequency and softening of stool texture while creating stronger odors. The supplements to take are numerous and for life. A cessation of these can be very dangerous. It will be necessary to demonstrate good motivation, and adequate understanding of the issues and an ability to manage supplements and follow-ups after the sleeve part.
POSSIBLE COMPLICATIONS
- - Bleeding
- - Infection
- - Stapled line or anastomotic leak
- - Connector leaks
- - Gastroesophageal relax disease
- - Peritonitis (abdominal infection)
- - Stricture of the stomach (stenosis)
- - Internal hernias
- - Dumping syndrome
- - Cardiopulmonary complication or trombembolic
- - Malnutrition, vitamin, protein or micronutrient deficiencies
Revision surgeries include a set of procedures that can be applied to a set of different clinical situations that will need to be individualized to each patient. They include gastric band excision, conversion of gastric band to vertical gastrectomy or gastric bypass, conversion of vertical gastric bypass to gastric bypass or trillion-pancreatic bypass, or revision of vertical gastrectomy that is too large or problematic post gastric bypass. The explanations will be individualized for each patient. Please note that not all patients are candidates for revision surgery.
POSSIBLE COMPLICATIONS
- - Bleeding
- - Infection
- - Stapled line or anastomotic leak
- - Peritonitis (abdominal infection)
- - Stricture of the stomach (stenosis)
- - Internal hernias
- - Dumping syndrome
- - Cardiopulmonary complication or trombembolic
- - Malnutrition, vitamin, protein or micronutrient deficiencies
- - Stool changes like diarrhea and constipation
- - Gastroesophageal reflux disease